Stick a patch on your skin and let it do the work. That’s the pitch behind transdermal delivery, and it’s been popping up everywhere — from nicotine patches back in the ’90s to the wave of “wellness patches” that now clutter your Instagram feed. Some of them genuinely work. Plenty don’t. And the gap between those two categories keeps widening as the marketing sprints ahead of the science.
The transdermal drug delivery market hit roughly $35 billion in 2024, and projections have it climbing past $59 billion by 2034. Money like that doesn’t flow into a space without real demand. People want alternatives to needles and pills, and for certain molecules the technology does deliver. The trouble starts when brands stick the word “transdermal” on a product that couldn’t get its ingredients past the top layer of your skin if you wore it for a month.
Your Skin Doesn’t Want to Let Things In
Skin’s entire purpose is to be a barrier. It’s spectacularly good at it. The outermost layer — the stratum corneum — is a wall of dead cells packed with lipids, and virtually nothing gets past it without a fight.
Dermatologists Jan Bos and Marcus Meinardi sorted this out back in 2000 with a paper in Experimental Dermatology that gave us what’s now called the “500 Dalton rule”. Pretty straightforward: if a molecule weighs more than roughly 500 Daltons, it’s not crossing intact skin on its own. Every transdermal drug that works through passive absorption? Under that line. Every common contact allergen? Under it too. Over two decades later, the rule still holds.
To give you an idea of how this plays out:
| Molecule | Weight (Daltons) | Gets Through Skin? |
|---|---|---|
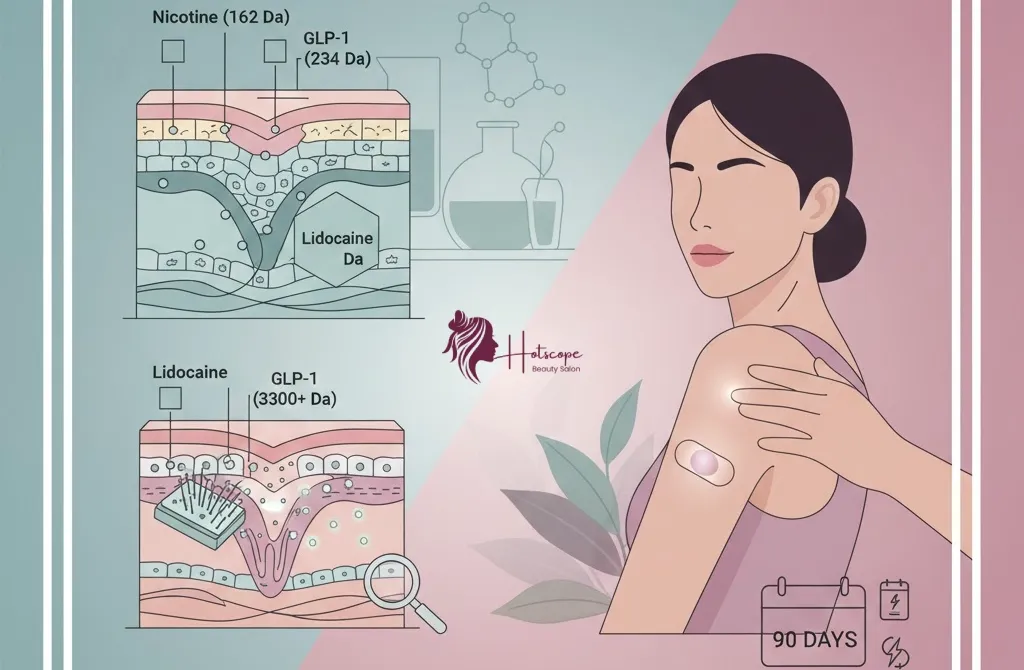
| Nicotine | ~162 Da | Yes |
| Vitamin C (ascorbic acid) | ~176 Da | Yes |
| Lidocaine | ~234 Da | Yes |
| Estradiol (estrogen) | ~272 Da | Yes |
| Retinol | ~286 Da | Yes |
| Berberine | ~336 Da | Poorly, needs help |
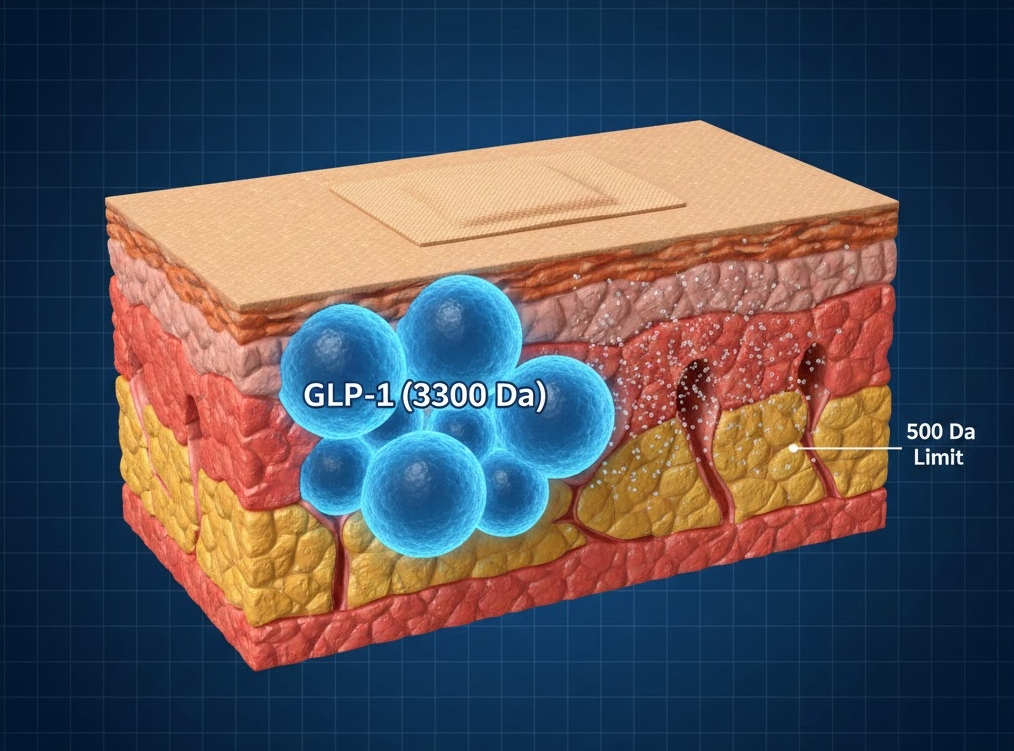
| GLP-1 peptide | ~3,300+ Da | No |
Keep an eye on that last row. It’s about to become very relevant.
Patches That Actually Do What They Claim
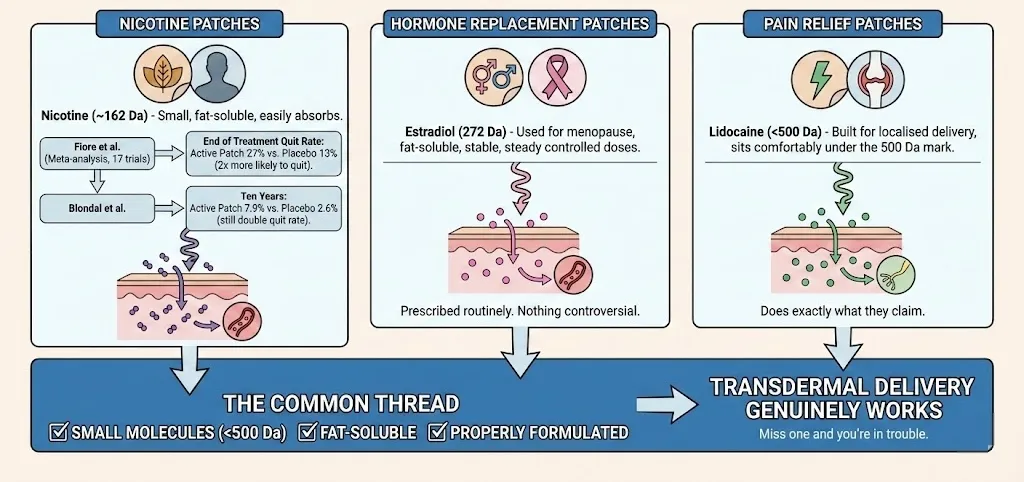
Nicotine patches are probably the best-known example of transdermal delivery done right. Nicotine weighs about 162 Da — well within the safe zone — and it absorbs through skin without much trouble. Fiore et al. ran a meta-analysis across 17 double-blind trials and found patch users were more than twice as likely to quit smoking as the placebo group, with abstinence at 27% versus 13% at end of treatment. A later study by Blondal et al. tracked people out to ten years — ten years — and the active patch group still had double the quit rate: 7.9% versus 2.6%.
Hormone replacement patches work for the same basic reasons. Estradiol — used for menopause symptoms — is 272 Da, fat-soluble, and stable enough to cross skin in steady controlled doses. These are prescribed routinely. Nothing controversial about them.
Pain relief patches using lidocaine sit comfortably under the 500 Da mark too. Built for localised delivery, and they do exactly what they claim.
The common thread across all of them: small molecules, fat-soluble, properly formulated. Tick those boxes and transdermal delivery genuinely works. Miss one and you’re in trouble.
Microneedles Are Worth Watching
Once you go above 500 Da, passive absorption is essentially dead. But researchers have been trying to find ways around that limit, and microneedle patches are the most promising route they’ve come up with.
Picture an array of tiny projections — usually between 100 and 1,000 micrometres long — that poke through just the outermost skin layer and create temporary microchannels. They’re too short to reach your nerve endings, so you barely feel them going in. And because they physically punch past the stratum corneum, they can carry larger molecules through a barrier that would otherwise block them completely.
Sánchez-Trasviña et al. put out a review in 2024 examining microneedle patches specifically for anti-obesity drug delivery. Their finding: the technology has real potential, including for GLP-1 analogs in animal models, but consumer-ready versions are still early days. Separately, researchers at Nanjing University of Chinese Medicine reviewed polymeric microneedle systems that same year and found they can significantly boost delivery efficiency for peptides, vaccines, and larger actives compared to standard patches.
You can already find microneedle patches for hyaluronic acid, vitamin C, and salicylic acid on beauty shelves. Some of them look genuinely promising for targeted delivery — wrinkle reduction, acne, brightening. But quality is all over the place. The engineering behind a properly made microneedle patch is complex, and cheap versions often don’t penetrate deep enough or dissolve too quickly to deliver anything useful.
GLP-1 Patches: The Science Hasn’t Caught Up to the Marketing
GLP-1 receptor agonists — Wegovy, Ozempic, Mounjaro — are genuinely effective weight-loss drugs when delivered by injection. Clinical trials show 15–25% body weight reduction. That evidence is rock solid.
Here’s the problem. GLP-1 is a peptide hormone weighing around 3,300 Daltons. Almost seven times over the 500 Da threshold. It’s water-soluble. Skin enzymes break it down. Getting this molecule through intact skin with a basic adhesive patch isn’t just hard — there is zero published evidence showing it works.
And yet the rise of GLP-1-based weight-loss patches has created a huge gap between what consumers are hoping for and what the science actually supports. Most products sold as “GLP-1 patches” don’t even contain GLP-1. They’re stuffed with herbal extracts — berberine, green tea, chromium, B-vitamins — and claim to “support natural GLP-1 production.” Berberine is the most studied of those ingredients, and even that only has evidence for modest blood sugar effects when taken orally at 1,000–1,500 mg per day.
In practice, this means berberine is typically consumed as a capsule or tablet rather than delivered through the skin. Some supplements, such as WOWMD Berberine Essentials, provide berberine in oral form within the dosage ranges commonly examined in metabolic health research. However, there is no published evidence showing berberine absorbs meaningfully through a small adhesive patch, which is why most studies focus on oral supplementation instead of transdermal delivery.
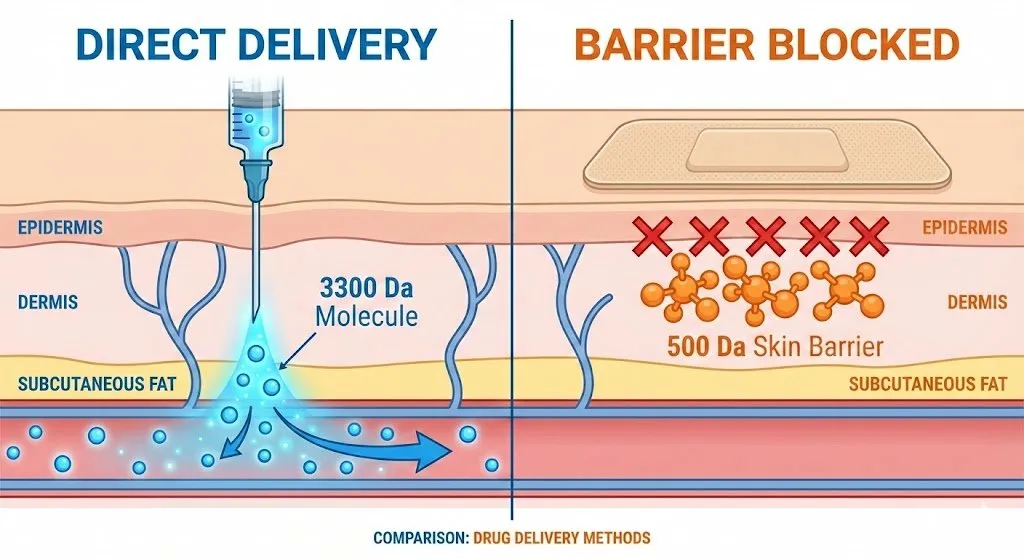
No FDA-approved GLP-1 patch exists. No MHRA-approved one either. Researchers are working on microneedle-based systems that might deliver GLP-1 analogs through the skin one day, and some animal work looks encouraging. But we’re talking lab-grade devices with sophisticated engineering behind them — a different universe from the consumer patches selling for £20 on Amazon.
Why Most Wellness Patches Fall Short
Molecule size gets most of the conversation, but it’s only one piece. A transdermal system needs several things working together to actually deliver ingredients into your body.
Fat solubility matters. The stratum corneum is rich in lipids, which means fat-soluble compounds slip through more easily. Plenty of the botanical extracts and vitamins marketed in wellness patches are water-soluble, and that’s a problem from the start.
You need enough of the active ingredient. Diffusion relies on having a high concentration on the patch side to push molecules through the skin. Consumer patches almost never disclose their ingredient doses, but the amounts are almost certainly way below what clinical studies use for oral delivery — and oral is already a more efficient absorption route.
Stability is a real issue. Peptides degrade. Skin enzymes chew through them. Heat, moisture, and time all eat away at potency. Something that works perfectly in a fresh injection might be useless after sitting in adhesive against your warm skin for half a day.
Where you stick it also counts. Skin thickness varies across your body. Thinner spots like the inner arm absorb better than thicker areas on your back or legs. Most consumer patches don’t bother telling you any of this.
All of these factors compound each other. A molecule might be small enough on paper but tank on solubility. It might have the right properties but degrade before enough absorbs. Pharmaceutical companies spend years in formulation development working through exactly these problems for their prescription patches. The wellness brands? Most of them skip that step entirely.
Before You Buy Anything
If a product claims it can deliver a large peptide or protein through a basic adhesive patch — with no microneedles, no iontophoresis, no advanced delivery tech at all — be very sceptical. Smaller molecules like nicotine, caffeine, certain vitamins, and some skincare actives are realistic candidates for transdermal delivery. A 3,300 Da peptide is not.
Check whether there’s clinical data behind the specific formulation being sold. Not testimonials. Not unverified before-and-after photos. Published, peer-reviewed studies on that product’s transdermal delivery — not just on the ingredient when taken orally.
And pay attention to regulatory status. Pharmaceutical transdermal patches go through years of testing. Consumer wellness patches sit in a grey zone where claims don’t need clinical backing. That distinction makes a big difference to whether what you’re buying actually does anything.
What’s Coming Next
The science is moving, and some of it is genuinely exciting. Microneedle tech is being studied for vaccines, insulin delivery, anti-aging peptides, even cancer therapies. Chen et al. published a review this year covering advances across drug delivery, biosensing, and personalised medicine, and suggested microneedle technology could see widespread clinical use within the next few years.
Smart patches that adjust delivery in real time based on sensor feedback are already being developed. Dissolving microneedles that break down after releasing their payload are getting refined. There’s serious work happening.
But for the stuff you can actually buy right now? The patches that work are the ones built on decades of pharmaceutical research. Nicotine. Hormones. Specific pain meds. Everything else falls somewhere between “interesting lab results” and “wishful thinking wrapped in good branding.”
Your skin is exceptionally good at its job. That’s worth remembering next time someone tries to sell you a sticker that promises otherwise.